Speaking as a Canadian, I have a significant beef with the current federal government and their so-called ‘experts’. It is my opinion that they have demonstrated complete incompetence from the earliest warnings that COVID-19 was an imminent threat to Canadians, and their totally inadequate response to it.
According to ABC News, “As far back as late November, U.S. intelligence officials were warning that a contagion was sweeping through China’s Wuhan region, changing the patterns of life and business and posing a threat to the population,”
“At the end of December, several weeks into a mysterious disease outbreak that was only starting to gain attention, an ophthalmologist in China’s central city of Wuhan sounded a stark warning. “A new coronavirus infection has been confirmed and its type is being identified. Inform all family and relatives to be on guard,” Li Wenliang typed into a chat group with his former medical school classmates on Dec. 30, 2019, according to Caixin, a Beijing-based media group. [But, alas, no freedom of speach in China.] Soon, Li’s message would resonate much farther. As the spiralling crisis emerged, he came to be known as the whistleblower of a virus that ultimately took his life.”
In a Reuters’ report it was noted that Taiwan initiated screening passengers arriving from China by air on December 31, 2019, the same day they contacted the WHO for information on the virus breakout in China. “Health Minister Chen Shih-chung, sitting next to Chou, said Taiwan had fortunately decided that same day to begin screening passengers flying in from Wuhan, and activated its emergency operations center on Jan. 2, 2020 – a move experts say allowed Taiwan to effectively control the early spread of the virus.”
While Taiwan did send experts to China in January, they were not allowed to see any patients or to go to the market where the virus is believed to have originated, Chen said. That trip made Taiwanese officials realize they had to act quickly.
China confirmed human-to-human transmission on Jan. 20. The WHO said on Jan. 12 there was no clear evidence of human-to-human transmission.”
Because of Taiwan’s preparedness and the prompt implementation of their Emergency Response Plan (which included 124 discreet action items including travel restrictions), with a population of 23.78 million, as of today, they only have 429 confirmed cases (1 infection per 55,400 people) and 6 deaths (one death per 4 million people).
The glaring question that needs to be answered is, why didn’t the WHO (and Canada) follow Taiwan’s lead? Is this not a case of astounding competence versus total incompetence?
On December 31, 2019 the WHO were first notified by China: “…the WHO China Country Office was informed of cases of pneumonia unknown etiology (unknown cause) detected in Wuhan City, Hubei Province of China. From 31 December 2019 through 3 January 2020, a total of 44 case-patients with pneumonia of unknown etiology were reported to WHO by the national authorities in China. During this reported period, the causal agent was not identified.” The WHO issued their first Situation Report three weeks later, on January 21, 2020.
Politico wrote, “Without China’s deceit and WHO’s solicitude for Beijing, the outbreak might have been more limited, and the world at the very least would have had more time to react to the virus. China committed unforgivable sins of commission, affirmatively lying about the outbreak and punishing doctors and disappearing journalists who told the truth, whereas the WHO committed sins of omission—it lacked independence and courage at a moment of great consequence.”
“On Jan. 14, WHO tweeted that “preliminary investigations” by Chinese authorities had found no evidence of human-to-human transmission of the coronavirus. Several days later, it reported “limited” human-to-human transmission, although it downplayed the finding as typical of respiratory illnesses. So, the WHO endorsed China’s narrative during the crucial early days of its cover-up.”
On January 30, 2020 the WHO was still not recommending active screening of passengers from other countries.
Politico reported: ‘Then, the WHO declined to call the outbreak in China a public health emergency of international concern on Jan. 22, at the same time there were confirmed cases in Taiwan, Australia, Japan, Thailand, and South Korea. After the WHO finally declared the emergency, it proceeded to drag its feet on declaring a pandemic, waiting until March 12.
Meanwhile, the WHO didn’t support restrictions on international travel. As a headline in Reuters put it in early February [February 3], “WHO chief says widespread travel bans not needed to beat China virus.”**
In effect, China and the WHO worked together to expose the rest of the world to the virus, at the same time they downplayed its dangers.’
**Interesting to note that COVID was referred to by the media as the “China virus.” in January, 2020 and nobody complained back then about racial bias. Perhaps the US president was following their lead?
February 29, 2020 WHO continues to advise against the application of travel or trade restrictions to countries experiencing COVID-19 outbreaks.
CBC News reported, “At one of the recent daily ministerial media conferences, Health Minister Patty Hajdu said her first major briefing on the pandemic occurred in early January.”
Canada’s Chief Medical Officer has been criticized for having tunnel-vision as a consequence of doggedly following WHO guidelines [even when clearly wrong], and where she serves as an advisor on the WHO Emergency Committee.
At a time when there were 17,238 confirmed infections in China including 361 deaths, as well as 151 confirmed cases in 23 countries, on February 3, 2020, World Health Organization chief Tedros Adhanom Ghebreyesus said “…there was no need for measures that “unnecessarily interfere with international travel and trade”
March 18, 2020 the Government of Canada bars foreign nationals from all countries, except the U.S., from entering Canada via air travel. On March 20, non-essential travel was banned between Canada and the USA . Canada was still not implementing mandatory screening of passengers entering the country. Why did it take the Canadian government 50 days to follow Taiwan’s lead?
April 30, 2020, the WHO is recommending social distancing of only 3‘, “Maintain at least 1 metre (3 feet) distance between yourself and others.’
Now comes the question of what comes next?
This blog was initiated by the video presentation made by two California doctors. In a matter of a few days the video had garnered well over 4-million views on YouTube. It was then taken down for ‘breaching community guidelines’. Then on April 27, 2020, without providing any specific evidence, the ACEP and AAEM released the following concerning the presentation made by the two doctors:
ACEP-AAEM Joint Statement on Physician Misinformation
The American College of Emergency Physicians (ACEP) and the American Academy of Emergency Medicine (AAEM) jointly and emphatically condemn the recent opinions released by Dr. Daniel Erickson and Dr. Artin Massihi. These reckless and untested musings do not speak for medical societies and are inconsistent with current science and epidemiology regarding COVID-19. As owners of local urgent care clinics, it appears these two individuals are releasing biased, non-peer reviewed data to advance their personal financial interests without regard for the public’s health.
COVID-19 misinformation is widespread and dangerous. Members of ACEP and AAEM are first-hand witnesses to the human toll that COVID-19 is taking on our communities. ACEP and AAEM strongly advise against using any statements of Drs. Erickson and Massihi as a basis for policy and decision making.
The controversial video can still be viewed on other sites. The two doctors did make some errors in their presentation but much of what they said is grounded in reality.
Observations and investigation of ‘facts’:
- The doctors have been accused of ‘shoddy statistics and false claims’. Is this true? From what I have seen, in the doctor’s use of statistics and their extrapolations, they have actually provided a worst-case scenario by applying the current results of COVID-19 testing and infection rates to all of California.
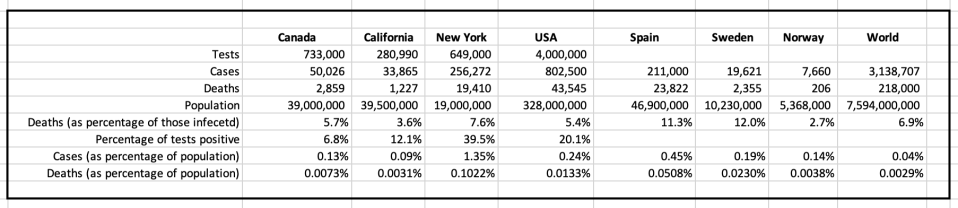
- Presently, 0.09% of Californians (33,865 out of a population of 39.5 million) have tested positive, leaving 99.91% of the population either uninfected or asymptomatic.
- We can never know the actual (total) rate of infection without testing 100% of the population or, at a minimum, testing a very large random sample of the population and the testing would only provide a snapshot at that moment in time. Extensive antibody testing would be the only way to accurately determine the total number of individuals who had been infected. So, it seems, even the ‘experts’ are guesstimating the status of COVID-19 around the world.
- We do know the death rate attributed to COVID-19, but only including comorbidities (significant underlying medical conditions), not without. Is this a critical failure in understanding the general impact of COVID-19?
- We can know the rate of hospitalization (although this is not currently publicized).
- Presently, in Canada, approximately 79% of new COVID deaths are within locations that care for the aged. Consequently, total deaths have doubled in the past three weeks.
- As a rule, of the general population, one in four Canadians will die in a nursing home, and of those, 70% will die in the nursing home, not a hospital.
- In a 2018 study of 690 participants, it was noted that the average life expectancy in a senior’s residence is 2.2 years, with a death rate of 31.8% per year. In another study of 8,433 participants, 53% died within 6 months of nursing home admission. Given such a high end-of-life fatality rate, what is the real impact of COVID-19 infections amongst residents of senior care facilities? This needs to be quantified. How do the numbers compare to common influenza outbreaks in nursing homes?
- The statement was made by the doctors: “COVID didn’t kill them, 25 years of tobacco use killed.” This is somewhat analogous to asking the question, ‘What killed the person, the shooter, the gun, or the bullet?’ Surely, the premeditation of the shooter was the cause of the killing. In the same way, 25-years of smoking was the ‘premeditation’ and COVID was the bullet. The two cannot be separated and yet COVID is almost exclusively reported as the cause of death. Is this appropriate?
- The doctors talk at some length about isolation negatively impacting our immune systems. NASA research would seem to back up much of what they said. Immune System Dysregulation During Spaceflight: “The immune system is highly sensitive to different types of stressors—psychological, physical, and local environmental (e.g., oxidative and radiation exposure). In healthy individuals, the flexibility and resilience of the immune system allow rapid recovery with little or no adverse effects. Yet, with high intensity and/or duration of extremes in environment, disrupted circadian rhythms, altered nutrition, and other factors that impact both physiological and psychological stress, adverse consequences to the immune system can occur (5–7). Environment, often considered as a combination of multiple “environmental exposures,” is defined as a “non-genetic” factor in the broad sense and is one of the three fundamental components of precision medicine: lifestyle, environment, and genetics (8). Autoimmunity, allergy, chronic infection, and other chronic diseases develop predominantly from a combination of environmental exposures with restrained genetic background influences.”
- The WHO states, “Worldwide, these annual [influenza] epidemics are estimated to result in about 3 to 5 million cases of severe illness, and about 290,000 to 650,000 respiratory deaths.” This extrapolates to a death rate of ‘serious’ incidents of 13%. The actual incidence of influenza is unknown and/or unreported.
- The WHO identifies the infection mortality rate for influenza, worldwide, is 0.1%. Referencing note 11., this would indicate that 1 case in 130 is severe, and from this, we can deduce that there are approximately 650 million cases of influenza each year, or 0.09% of the world’s population (which, coincidentally, is identical to the COVID infection rate quoted for California).
- The asymptomatic rate for influenza varies greatly from study to study, but the distillation of many studies would indicate a rate of 16%.
- The New England Journal of Medicine reports that the largest study concerning the asymptomatic rate for COVID-19, conducted thus far, has been in Iceland. In this study 13.3% of those tested were asymptomatic. They also noted that “The percentage of infected participants that was determined through population screening remained stable for the 20-day duration of screening.”
- Sweeping testing of the entire crew of the coronavirus-stricken U.S. aircraft carrier Theodore Roosevelt revealed and asymptomatic rate of 60%, but it should be noted that this is not a typical real-world environment.
- The global death rate from influenza types A and B is +/- 2% of all respiratory deaths, with 67% of these deaths being attributed to individuals 65 years or older.
- In the USA central reporting of deaths from influenza is not a requirement, so organizations such as the CDC can only guesstimate actual death rates. While it is reported that the death rate from influenza is 0.1% (or the refrain of COVID death rates being 10 times that of influenza) I could find no meaningful data to support these conclusions.
- Of critical importance to understand is the transmissibility of COVID. The New England Journal of Medicine notes, “What explains these differences in transmission and spread? A key factor in the transmissibility of Covid-19 is the high level of SARS-CoV-2 shedding in the upper respiratory tract,1even among pre-symptomatic patients, which distinguishes it from SARS-CoV-1, where replication occurs mainly in the lower respiratory tract.2Viral loads with SARS-CoV-1, which are associated with symptom onset, peak a median of 5 days later than viral loads with SARS-CoV-2, which makes symptom-based detection of infection more effective in the case of SARS CoV-1.3 With influenza, persons with asymptomatic disease generally have lower quantitative viral loads in secretions from the upper respiratory tract than from the lower respiratory tract and a shorter duration of viral shedding than persons with symptoms,4 which decreases the risk of transmission from pauci-symptomatic persons (i.e., those with few symptoms).”
- Artin Massihi, MD Artin Massihi is a Board Certified Emergency Room Physician. Emergency Physicians are qualified to diagnose, assess, and treat patients with acute trauma, illness and other life-threatening conditions. Dr Massihi has worked in level 1 as well as Level 2 trauma centers in many Emergency Rooms in the Los Angeles and Kern County regions. He received his undergraduate degree at the University of California at Irvine and attended Medical School at Loma Linda University. He then pursued internship training in General Surgery at the University of Southern California, and residency training in Emergency Medicine and Trauma at Kern Medical Center, an affiliate of the University of California at Los Angeles. Dr Massihi is also an Entrepreneur. He and his business partner Dr Daniel Erickson own the Accelerated Health Franchise, consisting of Accelerated Urgent Care, Accelerated Occupational Health and Accelerated Family Medicine. They have facilities throughout multiple cities and counties in the state of California. Dr Massihi is a fellow of the American Academy of Emergency Medicine and a proud member of the Armenian American Medical Society. He is also passionate about the Armenian Cause and helping those less fortunate globally.
- Daniel Erickson, DO is an emergency medicine specialist in Bakersfield, CA and has been practicing for 20 years. He graduated from Western Univ Of Health Sciences/College Of Osteopathic Medicine Of The Pacific, Western University Of Health Sciences in 2004 and specializes in emergency medicine.
What follows is a transcript of the presentation made by Dr. Erickson and Dr. Artin Massihi (it does not include the Q&As).
The transcript has been broken down into individual statements (given as fact), general questions and hypothetical questions.
Notes inserted [in red] were later clarifications or [corrected errors] in response to the Q&A session.
During the presentation Dr. Erickson and Dr. Massihi make 100+ statements, ask 18 general questions and 8 hypothetical questions:
“We’d like to look at how we’ve responded as a nation, and why you responded.
- Our first initial response two months ago was a little bit of fear: [the government] decided to shut down travel to and from China. These are good ideas when you don’t have any facts.
- [Governments] decided to keep people at home and isolate them. Typically, you quarantine the sick. When someone has measles, you quarantine them. We’ve never seen where we quarantine the healthy.
So that’s kind of how we started.
- We don’t know what’s going on, we see this new virus.
[QUESTION]: How should we respond?
- So, we did that initially, and over the last couple months we’ve gained a lot of data typically.
- We’re going to go over the numbers a little bit to kind of help you see how widespread COVID is and see how we should be responding to it based on its prevalence throughout society—or the existence of the cases that we already know about….
- So, if you look at California—these numbers are from yesterday—we have 33,865 COVID cases, out of a total of 280,900 total tested. That’s 12% of [those tested, as later clarified] Californians were positive for COVID.
- So, we don’t, the initial—as you guys know, the initial models were woefully inaccurate. They predicted millions of cases of death—not of prevalence or incidence—but death. That is not materializing.
- What is materializing is, in the state of California is 12% positives [of those tested, as later clarified].
- You have a 0.03 chance of dying from COVID in the state of California [based on 1,227 deaths, as later clarified, or 3 per 100,000 of the population].
HYPOTHETICAL QUESTION: Does that necessitate sheltering in place? Does that necessitate shutting down medical systems? Does that necessitate people being out of work?
- 96% of people in California who get COVID would recover [without intervention or hospitalization], with almost no significant sequelae; or no significant continuing medical problems. Two months ago, we didn’t know this.
- The more you test, the more positives you get. The prevalence number goes up, and the death rate stays the same. So [the death rate] gets smaller and smaller and smaller. And as we move through this data—what I want you to see is—millions of cases, small death. Millions of cases, small death.
- We extrapolate data, we test people, and then we extrapolate for the entire community based on the numbers.
- The initial models were so inaccurate they’re not even correct.
- And some of them [initial models] were based on social distancing and still predicted hundreds of thousands of deaths, which has been inaccurate.
- In New York the ones they tested they found 39% positive.
HYPOTHETICAL QUESTION: So, if they tested the whole state would we indeed have 7.5 million cases? We don’t know; we will never test the entire state.
- So, we extrapolate out; we use the data we have because it’s the most we have versus a predictive model that has been nowhere in the ballpark of accurate.
- How many deaths do they have? 19,410 out of 19 million people, which is a 0.01% chance [should be 0.1%, and is 10 times the national average] of dying from COVID in the state of New York.
- If you are indeed diagnosed with COVID-19, 92% of you will recover [without intervention or hospitalization].
- We’ve tested over 4 million… which gives us a 19.6% positive out of those who are tested for COVID-19.
HYPOTHETICAL STATEMENT: So, if this is a typical extrapolation [based upon test data] 328 million people times 19.6 is 64 million. That’s a significant amount of people with COVID; it’s similar to the flu. [US national COVID death rate is currently 0.0133% of the population]
- If you study the numbers in 2017 and 2018, we had 50 to 60 million with the flu. And we had a similar death rate in the deaths the United States were 43,545—similar to the flu of 2017-2018. We always have between 37,000 and 60,000 deaths in the United States, every single year. No pandemic talk. No shelter-in-place. No shutting down businesses…
- We do thousands of flu tests every year. We don’t report every one, because the flu is ubiquitous and to that note we have a flu vaccine.
[QUESTION:] How many people even get the flu vaccine?
- The flu is dangerous, it kills people. Just because you have a vaccine doesn’t mean it’s going to be everywhere, and it doesn’t mean everyone’s going to take it…
[HYPOTHETICAL] I would say probably 50% of the public doesn’t even want it. Just because you have a vaccine—unless you forced it on the public—doesn’t mean they’re going to take it.
- Norway has locked down; Sweden does not have lock down.
[QUESTION:] What happened in those two countries? Are they vastly different?
[QUESTION:] Did Sweden have a massive outbreak of cases?
[QUESTION:] Did Norway have nothing?
Let’s look at the numbers.
- Sweden has 15,322 cases of COVID—21% of all those tested came out positive for COVID. [April 29 20,302 cases and 2,462 deaths.]
- What’s the population of Sweden? About 10.4 million.
- So, if we extrapolate out the data about 2 million cases of COVID in Sweden. They did a little bit of social distancing; they would wear masks and separate; they went to schools; stores were open. They were almost about their normal daily life with a little bit of social distancing. They had how many deaths? 1,765.
- California’s had 1,220 with isolation.
- [Sweden] No isolation: 1,765. We have more people. Norway: its next-door neighbor. These are two Scandinavian nations; we can compare them as they are similar. 4.9% of all COVID tests were positive in Norway. Population of Norway: 5.4 million. So, if we extrapolate the data, as we’ve been doing, which is the best we can do at this point, they have about 1.3 million cases. Now their deaths as a total number, were 182. So, you have a 0.003 chance of death as a citizen of Norway and a 97% recovery. Their numbers are a little bit better. Does it necessitate shutdown, loss of jobs, destruction of the oil company, furloughing doctors? [April 29 7,660 cases and 206 deaths.]
[Note: % of population infected with COVID-19: Norway 0.14%, Sweden 0.19%. Deaths (as percentage of those infected): Norway 2.7%, Sweden 12%.]
I wanted to talk about the effects of COVID-19, the secondary effects.
- COVID-19 is one aspect of our health sector.
[QUESTION:] What has it caused to have us be involved in social isolation?
[QUESTION:] What does it cause that we are seeing the community respond to?
- Child molestation is increasing at a severe rate.
- We could go over multiple cases of children who have been molested due to angry family members who are intoxicated, who are home, who have no paycheck.
- Spousal abuse: we are seeing people coming in here with black eyes and cuts on their face. It’s an obvious abuse of case.
- These are things that will affect them for a lifetime, not for a season. Alcoholism, anxiety, depression, suicide. Suicide is spiking; education is dropped off; economic collapse.
- [In the] Medical industry we’re all suffering because our staff isn’t here, and we have no volume. We have clinics from Fresno to San Diego and these things are spiking in our community. These things will affect people for a lifetime, not for a season.
- I’d like to go over some basic things about how the immune system functions, so people have a good understanding.
- The immune system is built by exposure to antigens: viruses, bacteria.
- When you’re a little child crawling on the ground, putting stuff in your mouth, viruses and bacteria come in. You form an antigen antibody complex. You form IgG IgM. This is how your immune system is built.
- You don’t take a small child put them in bubble wrap in a room and say, “go have a healthy immune system.”
- This is immunology, microbiology 101.
- This is the basis of what we’ve known for years.
- When you take human beings and you say, “go into your house, clean all your counters—Lysol them down you’re going to kill 99% of viruses and bacteria; wear a mask; don’t go outside.”
[Question] What does it do to our immune system? [Reference Comment 10. above]
- Our immune system is used to touching.
- We share bacteria. Staphylococcus, streptococcal, bacteria, viruses.
- Sheltering in place decreases your immune system.
[HYPOTHETICAL QUESTION]: And then as we all come out of shelter in place with a lower immune system and start trading viruses, bacteria—what do you think is going to happen?
- Disease is going to spike.
- And then you’ve got diseases spike—amongst a hospital system with furloughed doctors and nurses.
- This is not the combination we want to set up for a healthy society. It doesn’t make any sense.
[HYPOTHETICAL QUESTION]: …Did we respond appropriately?
- Initially the response, fine shut it down, but as the data comes across—and we say now, wait a second, we’ve never, ever responded like this in the history of the country why are we doing this now?
- Any time you have something new in the community medical community it sparks fear—and I would have done what Dr. Fauci did—so we both would have initially.
- Because the first thing you do is, you want to make sure you limit liability—and deaths—and I think what they did was brilliant, initially.
- But you know, looking at theories and models—which is what these folks use—is very different than the way the actual virus presents itself throughout communities….
- Nobody talks about the fact that coronavirus lives on plastics for three days and we’re all sheltering in place. Where’d you get your water bottles from? Costco. Where did you get that plastic shovel from? Home Depot.
- If I swab things in your home, I would likely find COVID-19.
- And so, you think you’re protected.
[QUESTION:] Do you see the lack of consistency here?
[QUESTION:] Do you think you’re protected from COVID when you wear gloves that transfer disease everywhere?
- Those gloves have bacteria all over them.
- We wear masks in an acute setting to protect us.
[QUESTION]: We’re not wearing masks. Why is that? Because we understand microbiology; we understand immunology; and we want strong immune systems.
- I don’t want to hide in my home, develop a weak immune system, and then come out and get disease.
- When someone dies in this country right now, they’re not talking about the high blood pressure, the diabetes, the stroke. They say they died from COVID.
- We’ve been to hundreds of autopsies. You don’t talk about one thing; you talk about comorbidities.
- COVID was part of it, it is not the reason they died folks.
- When I’m writing up my death report, I’m being pressured to add COVID.
[QUESTION]: Why is that? Why are we being pressured to add COVID?
[HYPOTHETICAL QUESTION]: To maybe increase the numbers, and make it look a little bit worse than it is?
- We’re being pressured in-house to add COVID to the diagnostic list when we think it has nothing to do with the actual cause of death.
- The actual cause of death was not COVID, but it’s being reported as one of the disease processes and being added to the death list. COVID didn’t kill them, 25 years of tobacco use killed.
- There’s two ways to get rid of virus: either burns itself out or herd immunity.
- For hundreds of years we relied on herd immunity.
- Viruses kill people, end of story.
- The flu kills people.
- COVID kills people.
- But for the rest of us we develop herd immunity.
- We developed the ability to take this virus in and defeat it and for the vast majority 95% of those around the globe.
[HYPOTHETICAL QUESTION]: Do you want your immune system built or do you want it not built? [Reference comment 10. above]
- The building blocks of your immune system is a virus and bacteria.
- There are normal bacteria in normal flora that we have to be exposed to bacteria and viruses that are not virulent are our friends. They protect us against bad bacteria and bad viruses.
- Right now, if you look at Dr. Erikson’s skin or my skin, we have strep, we have stuff—they protect us against opportunistic infections.
- That’s why for the first three to six months [babies are] extremely vulnerable to opportunistic infection.
- Which is why, when we see a little baby in the ER with fever who is one month old, you do a spinal tap, you do a chest x-ray, you do blood cultures, you do urine cultures.
- But if you [adults] had a fever I wouldn’t do that for you.
- Why? Because that baby does not have the normal bacteria and flora from the community, whereas you do.
- I guarantee when we reopen there’s going to be a huge, huge amount of illness that’s going to be rampant because our immune systems have weakened. That’s just basic immunology.
[QUESTION]: Do we need to still shelter in place?
- Our answer is emphatically no.
[QUESTION]: Do we need businesses to be shut down?
- Emphatically no.
[QUESTION]: Do we need to have it, do we need to test them, and get them back to work?
- Yes, we do.
- The secondary effects that we went over—the child abuse, alcoholism, loss of revenue—all these are, in our opinion, a significantly more detrimental thing to society than a virus that has proven similar in nature to the seasonal flu we have every year.
- We also need to put measures in place so economic shutdown like this does not happen again.
- We want to make sure we understand that quarantining the sick is what we do, not quarantine the healthy.
- We need to make sure if you’re going to dance on someone’s constitutional rights you better have a good reason.
- You better have a really good scientific reason, and not just theory.
- One of the most important things is we need our hospitals back up.
- We need our furloughed doctors back.
- We need our nurses back.
- Because when we lift this thing, we’re going to need all hands on deck.
- I know the local hospitals have closed two floors.
- Folks, that’s not the situation you want.
- We’re essentially setting ourselves up to have minimal staff, and we’re going to have significant disease. That’s the wrong combination.
- I’ve talked to our local head of the Health Department and he’s waiting… for the powers that be to lift. Because the data is showing its time to lift.
- I would start slowly [open up schools sporting events] I think we need to open up the schools start getting kids back to the immune system you know and the major events the sporting events these are non-essential let’s get back to those slowly let’s start with schools let’s start with cafe Rio and the pizza place here…
[QUESTION]: Does that make sense to you guys and I think I can go into Costco and I can shop with people and there’s probably a couple hundred people, but I can’t go in Cafe Rio so big businesses are open little businesses are not….
- Eventually we treat this like we treat flu. Which is if you have the flu and you’re feeling fever and body aches you just stay home if you have coughing or shortness of breath—COVID is more of a respiratory thing—you stay home.
- You don’t get tested, even when people come with flu a lot of times, we don’t test them. We go, “you have flu. Here’s a medication.” You have COVID, go home, let it resolve and come back negative.
- If you have no symptoms you should be able to return to work.
[QUESTION]: Are you an asymptomatic viral spreader?
- Maybe, but we can’t test all of humanity.
- Sure, we’re going to miss cases of coronavirus, just like we miss cases of the flu.
- It would be nice to capture every coronavirus patient, but is that realistic?
[QUESTION]: Are we going to keep the economy shut down for two years and vaccinate everybody?
- That’s an unrealistic expectation.
- You’re going to cause financial ruin, domestic violence, suicide, rape, violence and what are you going to get out of it?
- You’re still going to miss a lot of cases.
- So, we need to treat this like the flu, which is familiar, and eventually this will mutate and become less and less virulent…
- I don’t need a double-blind clinically controlled trial to tell me if sheltering in place is appropriate, that is a college-level understanding of microbiology.
- A lot of times in medicine you have to make you have to make educated decisions with the data that you have.
- I can sit up in the 47th-floor in the penthouse and say we should do this, this, and this, but I haven’t seen a patient for 20 years—that’s not realistic.
- If you’re healthy and you don’t have significant comorbidities and you know you’re not immunodeficient and you’re not elderly, you should be able to go out without any gloves and without a mask.
- If you are those things you should either shelter in place or wear a mask and gloves.
- I don’t think everybody needs to wear the masks and gloves because it reduces your bacterial flora… and your bacterial flora and your viruses your friends that protect you from other diseases [if they] end up going away and now you’re more likely to get opportunistic infections that are hoping you don’t have your good bugs fighting for you.
